
The Ineffective Messaging of “Myocarditis in Young, Male Athletes"
Sudden Kidney Failure Exposes Poor Messaging

[The second article in a series — Thank you, Dr. Meryl Nass, for the recommendation to break this into multiple articles. Here are the likely articles in the series. 1) Leadership, Management, and Strategic Planning in the Covid Era, 2) The Ineffective Messaging of “Myocarditis in Young, Male Athletes”, 3) Sudden Kidney Failure Began with Government Incentives, not with COVID, 4) Top-Down Investigation, Bottom-Up Quantification Method for Epidemiological Vigilance, 5) Differences in Pneumonia, COVID, and All-Cause Death Profiles by Age Group.]
The main objective of this article is to raise awareness of four (4) years of missteps in strategic messaging from the health freedom movement. Many “leaders” in the movement focus on “myocarditis in young, male athletes” on podcasts and in articles and research papers. This article elucidates the folly of such a narrowly constrained message. If the objective is to get people to realize the true magnitude of deaths and injuries from COVID “vaccines,” then the myocarditis message acts adversely to that objective. The myocarditis message, by reference to the lived experiences of the great majority, suggests that serious COVID “vaccine” injury and death are “rare.” You will see the relative differences among causes of death in this article. Be sure to read the “weaknesses” section near the end of this article. Myocarditis is a major issue caused by COVID “vaccines.” It’s just not a mindshare winner as a message.
The issue of poor messaging
Imagine the following interaction. You mention that COVID “vaccines” cause clotting. Your friend then says, “My cousin was healthy and active at 47 years old and just dropped dead from a stroke. Do you think it had something to do with the COVID vaccine?” You are thankful people are finally considering this question and you calmly answer, “Yes, it is well-documented that COVID “vaccines” cause strokes.”
Messaging is the greatest issue facing the health freedom movement. Everything hinges on public opinion.
After four (4) years, the attribution of kidney failure, clotting, hemorrhaging, and cancer to the COVID “vaccines” has not sufficiently entered the public consciousness. If you ask anyone outside the health freedom movement what serious side effects might be caused by COVID gene drug “vaccines,” they will likely answer, “Well, I heard that myocarditis occurs in young, male athletes.” Many know only about this issue because the biggest voices in the health freedom movement repeatedly call out cases of “myocarditis in young, male athletes.”
News media consistently report that COVID “vaccine” associated deaths on athletic fields are “extremely rare.” Again, people are led to believe that one has to be male, young, and athletic to fall victim to COVID “vaccines.” The average person does not make the connection between COVID “vaccines” and deaths or new illnesses in their neighborhood, social circle, or extended family involving causes such as lymphoma, immune dysregulation, stroke, pulmonary embolism, and sudden kidney failure.
By the numbers
NOTE: The numbers herein are obtained from the U.S. government’s CDC Wonder found at https://wonder.cdc.gov/. The whole of the United States is included in these data sets. For the purposes of this article, “Myocarditis-involved” deaths are determined by adding quantities of deaths involving ICD (International Classification of Diseases) code “I40 Acute myocarditis” or code “I51.4 Myocarditis, unspecified.” Excess deaths are determined by 1) approximating a trend line through the actual numbers for years 2010 through 2019, 2) extending the trend line through subsequent years through 2024 in order to establish what was expected from 2020 through 2024, 3) subtract the expected number from the actual number for each time period to determine excess. [Excess = Actual - Expected; Expected (2020) = INTERCEPT(actual values from 2015-2019) + 5 * SLOPE(actual values from 2015-2019); Expected (2021) = … 6 * SLOPE …; Expected (2022) = … 7 * SLOPE…; repeat for 2023 and 2024; INTERCEPT and SLOPE use linear least squares algorithms to approximate a line among data points]
The following ICD codes and causes-of-death match the corresponding x-axis categories in the four (4) graphs:
I40 or I51.4 Myocarditis in young males ages 5 through 34 years old
I40 or I51.4 Myocarditis in all ages, both sexes
C77 Secondary and unspecified malignant neoplasm of lymph nodes
D8 Certain disorders involving the immune mechanism
I63 Cerebral infarction
I26 Pulmonary embolism
N17 Acute renal failure
In 2022, I began by obtaining all the electronic death records for the years 2015-2023 for Massachusetts, then obtained Vermont, Minnesota, and Connecticut from other parties. I was able to look at all the causes-of-death from before the COVID pandemic, during the year of the pandemic before vaccines were available (2020), and then during 2021-2023 when a reported 81% of the US population received at least one COVID vaccine.1 I learned that lymphoma, stroke, pulmonary embolism, acute kidney failure and immune dysregulation were listed as causes of death much more often after the vaccines rolled out, but NOT during 2020, when COVID raged through the United States. I then wrote two (2) books and more than 100 articles regarding my findings. Especially noteworthy is that 2020 was a year of greater excess respiratory deaths, while 2021 and thereafter were years of greater clotting and hemorrhaging excess deaths. Since diseases do not change how they kill on a year boundary, something other than COVID began killing people through blood and immune related disorders in January 2021, when COVID “vaccines” were introduced.
For this article, I brought my knowledge and experience gleaned from state death record analysis to the CDC Wonder database, which compiles all death records from the fifty (50) United States by cause-of-death, date-of-death, age, gender, and other variables.
Through my work in state death records, I knew where to find anomalies in the entire United States. For specific ICD codes, I then totaled deaths for each of years 2015 through 2023. From those totals, I calculated excess death totals from 2021 through 2023 by ICD code. The results in the four (4) graphs show the relative differences in excess quantities by cause-of-death.
Here are the results.
Needless message diminution using qualifiers

Figure 1
Figure 1 depicts a 10X diminution by application of the qualifiers “young,” “male,” and “athletes” to the broader category of myocarditis in all ages and both sexes. Why the “experts” restrict their speech to these qualifiers is no mystery. There are hundreds of extremely compelling stories and videos of athletes running on the field and dropping dead or having a seizure. College and professional games have videos from many angles, leading to great video documentation of the events. However, if all someone hears is that COVID “vaccines” cause “myocarditis in young, male athletes," then they will believe that COVID “vaccine” injury and death are “rare,” which is false.
Cancer and stroke look down upon myocarditis

Figure 2
Figure 2 puts in perspective the relative excess rates of deaths involving 1) myocarditis in young, male athletes, 2) myocarditis in all ages and both sexes, 3) lymph node cancer, and 4) cerebral infarction, or ischemic stroke. The latter two (2) are 28X and 42X greater than the highly constrained and ineffective message of “myocarditis in young, male athletes.”
PE and immunodeficiency disappear myocarditis
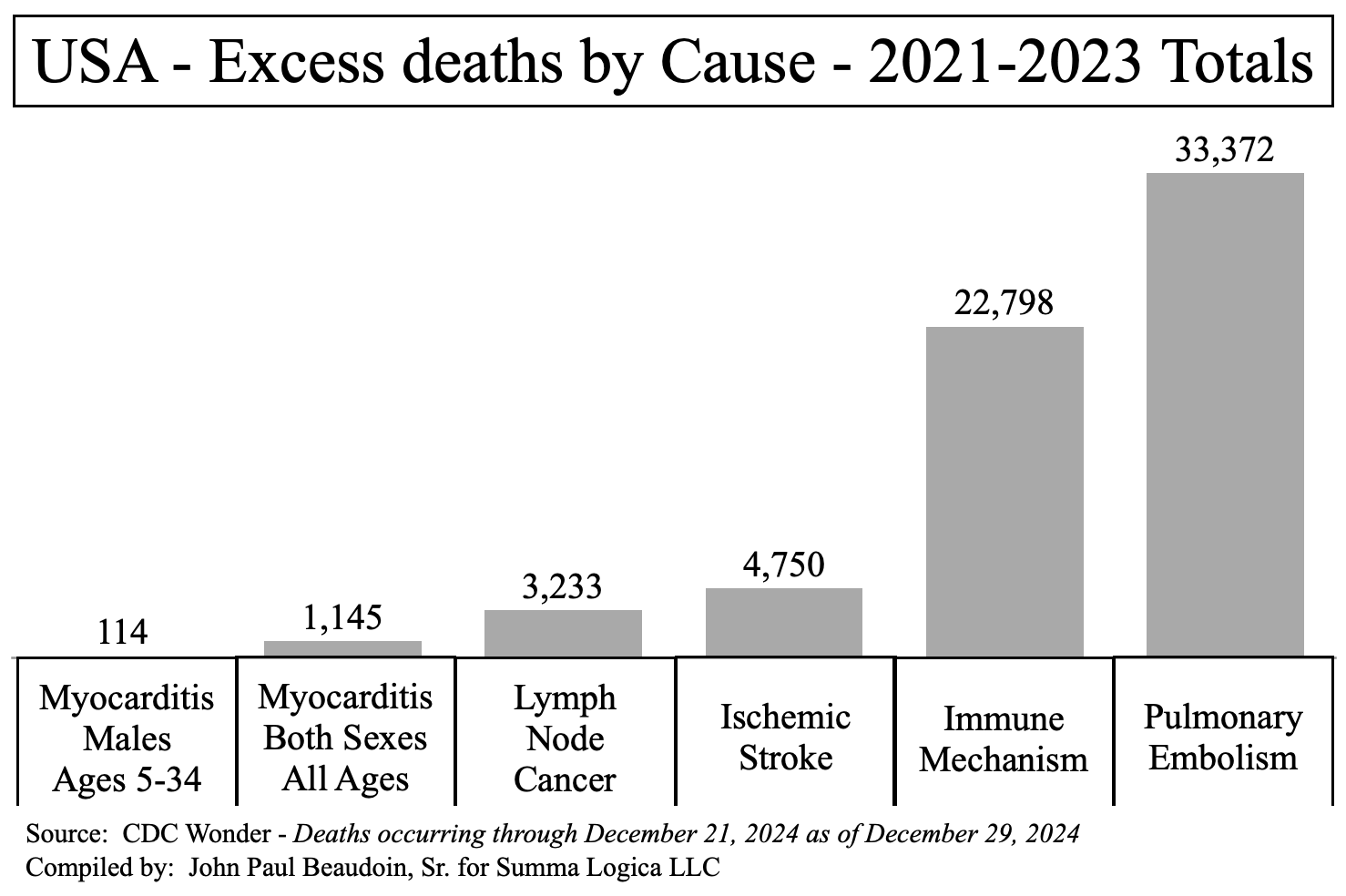
Figure 3
Figure 3 adds even greater perspective in the depiction of excess deaths involving the “Immune Mechanism” at 200X and "Pulmonary Embolism” at 293X the rate of excess deaths involving myocarditis in males ages 5 through 34 years old.
The reason I spend so much time talking and presenting about N17 Acute renal failure, aka Acute kidney injury (AKI), aka Sudden kidney failure will now become obvious. I sincerely hope that this article will make a positive difference in the way well-known health freedom experts speak about symptoms of injury and death caused by COVID “vaccines.”
An MD or PhD degree does not impart knowledge or experience in strategic messaging upon a physician or scientist. I hope they can at least learn the importance of strategic messaging from this article. Success or failure in war is not defined only by winning or losing. The casualty rate is also a significant determinant of success. Strategic planning and preparation reduce casualties and increase the chances of winning a war. Get your messaging right.
A holocaust ignored - AKI - sudden kidney failure
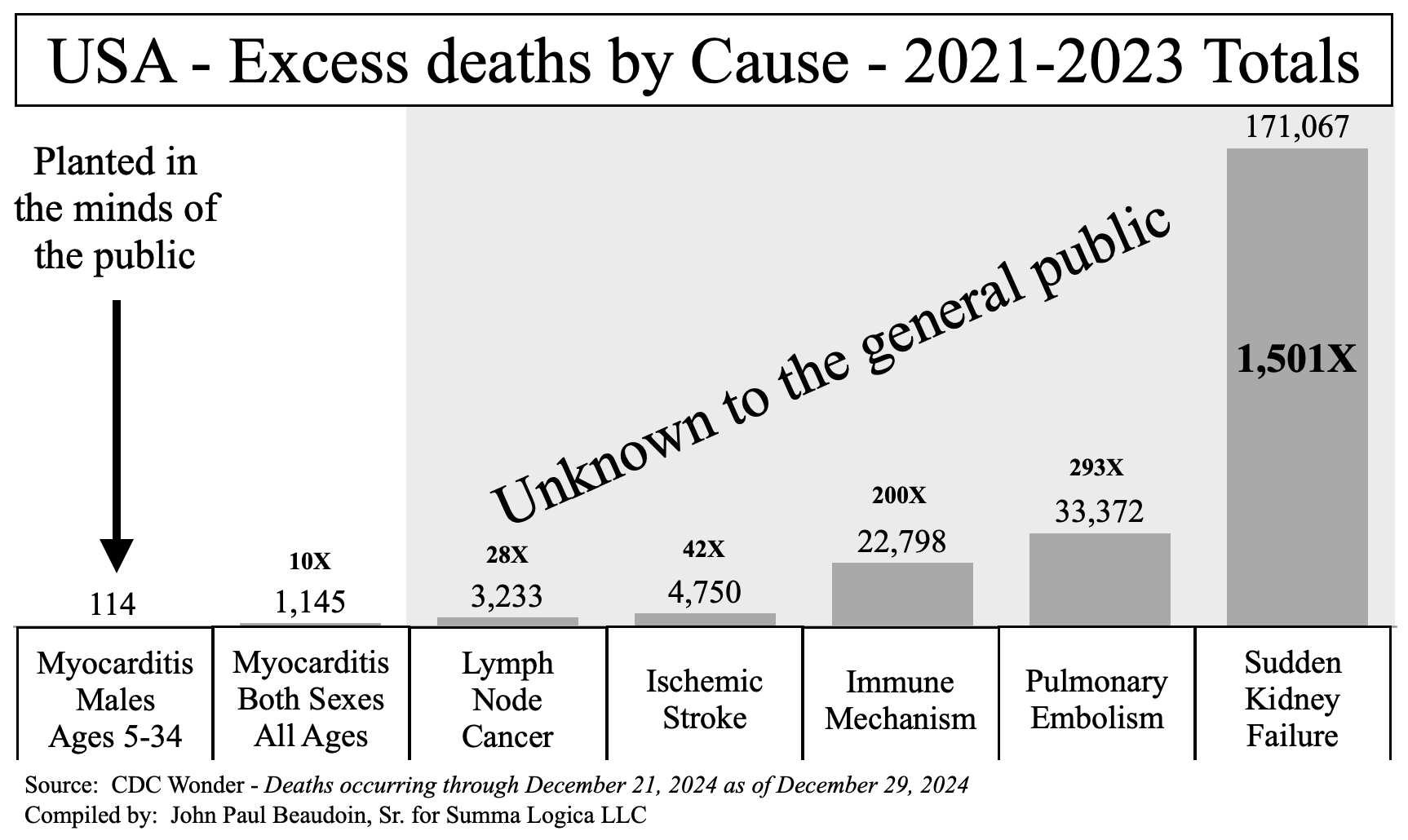
Figure 4
Figure 4 needs no explanation. Take time to study it. Yes, you are really seeing AKI in context. For more than two (>2) years of speaking, presenting, and writing about AKI, I had to listen to “leaders” of the health freedom movement unknowingly draw public opinion into a choke point — a “myocarditis in young, male athletes” mindshare kill zone that reduces attribution of death from COVID “vaccines” by more than a thousand fold (>1,000X).
The year 2024 brought more excess deaths in some, but not all causes. Excess N17 Acute renal failure involved deaths in 2021 through 2024 totals 211,802, adding another 40,735 in 2024, while no excess myocarditis-involved deaths occurred in 2024 to the date of this article.
Can we afford to continue poor and ineffectual messaging given the reality of Figure 4? Every pixel in the bars of those graphs represents a person who needlessly died as a result of government “recommendations.” Strong evidence supports the notion that government recommendations killed a million Americans in the COVID era.
The ability to win public opinion depends strongly on whether the average person encounters a death among their acquaintances, family, or friends from a cause they associate with the “vaccine.” If they hear about AKI instead of “myocarditis in young, male athletes,” the likelihood they would be personally impacted and make attribution of cause-of-death to “vaccine” would be 211,802 to 114, or 1,858 times more likely.
Legal Duty to Act
The leaders of the NIH, FDA, and CDC have a legal duty to ensure that an earnest and immediate forensic investigation occurs using the medical files from decedents who died from AKI. This effort would only take a few man-weeks for a pathologist or medical examiner. There is no excuse why these federal agencies have neither found nor mentioned that hundreds of thousands of Americans are dead from AKI due to an externality that began in November 2020 and another externality that began in late December 2020 or early January 2021 (timing to be depicted in the next article in this series).
Specific and credible evidence of imminent harm to the public is provided in this article. This article and the following documents are gleaned from official government records: Exhibit F from Beaudoin v Baker et al (2022)2 now at the First Circuit Court of Appeals; THE CDC MEMORANDUM (2024)3 sent certified mail to the directors of the CDC, NIH, FDA, and thirteen (13) of their deputy directors; and THE CONNECTICUT MEMORANDA SERIES Volumes I and II (2024)45 confirmed to have been received by the offices of Connecticut’s Governor Lamont, Attorney General Tong, Health Commissioner Juthani, and the Auditors of Public Accounts of Connecticut. The evidence referenced in these documents far exceeds the requisite reasonable belief and suspicion standard required to compel investigation per legal duty of government officials.
There are no excuses. The omission of investigation is a felony failure of required legal duty to act. The People are dying and demand answers from our governments.
Conclusions
COVID “vaccine” caused deaths involving AKI, pulmonary embolism, stroke, immune dysregulation, and turbo cancer should be the leading story in any conversation about COVID “vaccines.” Only after these are mentioned should you add “myocarditis, too” at the end of the conversation.
AKI is involved in 211,805 excess deaths (2021-2024) in the United States at ages far younger than those from COVID disease per se.
Strengths of conclusions
The greatest strength lies in the readers’ personal experiences involving the subject matter. The conclusion surrounding specific causes and their relative “rarity” (or commonness) will likely resonate with many readers who hear about myocarditis continually, but rarely hear about AKI.
The conclusions stand upon raw data, available to pedestrian readers and devoid of statistical inferences and tricks of probability functions. The graphs are compelling to, and understood by, people of all ages and vocations.
Weaknesses of conclusions
This article only accounts deaths, not injuries, which may diminish the importance of myocarditis.
Prevalence disparity - Myocarditis is far more relatively prevalent as injuries among the “vaccinated” than it is as deaths among the “vaccinated.”
Time-Delay - Myocarditis likely takes decades off the back-end of life of current youths and young adults. We may not know for decades if more “vaccinated” youngsters will die due to heart damage at 60 years old instead of 80 years old, a loss of 20 years.
Replacement Causes in the Susceptible - Elderly and late middle age adults, who are susceptible to react to COVID “vaccines,” perhaps die from a myocardial infarction (heart attack) hours before myocarditis has the opportunity to set in. Heart attacks were not counted in this article though they may pre-empt death in those who would otherwise die from myocarditis hours later. Or, very simply, myocarditis may be involved in most of these heart attacks right after the “vaccines,” but myocarditis is not listed because there was no autopsy.
Fraud and mistake in the recording and certification of deaths is proven to be common during the COVID era (see The Real CdC,6 THE CDC MEMORANDUM, THE CONNECTICUT MEMORANDA SERIES). Erroneous data is a significant weakness that underlies all vital records data. The only way to deal with fraud and mistake is to assume ceteris paribus conditions. In other words, you must assume that the same personnel are performing the same way over the period of time under scrutiny in the data study. However, ceteris paribus can be inconsistent across different causes-of-death. While acute renal failure, pulmonary embolism, and stroke are likely honest and accurate certifications, ambiguity in causes-of-death such as cardiac arrest, atrial fibrillation, and “influenza without a test” can cause fluctuations in accuracy of data due to temporary biases of the certifiers of death. For example, if thrombocytopenia is certified as a cause, then it is highly likely the person had thrombocytopenia because it is based on a laboratory report of platelet counts. However, if someone was found dead on their couch and no autopsy was done, it might be presumed that their heart just stopped, and they might be labeled “cardiac arrest.” Without an autopsy and series of blood labs, it cannot be certain that it was not food poisoning, low serum sodium, or some bacterial or blood issue.
Thank you for reading this article. The most important issue is that the governments are ignoring a mass casualty event greater than the fraud they purport COVID disease to have been. And part of the reason the governments are getting away with ignoring the mass casualty event is because the public is programmed to talk about “myocarditis in young, male athletes.”
THE END
God bless you all
John 14:6 TRUTH
References
First, here is a table from which graphs were derived. If anyone wants to look at totals, percentages of all-cause deaths, or other metrics, then they can use these numbers to do so. This can also be used to verify the excess deaths stated herein.

(2025). What’s the nation’s progress on vaccinations? US Coronavirus vaccine tracker. USAFACTS.org. Found at https://usafacts.org/visualizations/COVID-vaccine-tracker-states/ on 2025 January 08.
Beaudoin, J. P., Sr. v. Baker, C. D., et al. (2022). U.S. District Court, District of Massachusetts, Case No. 1:22-cv-11356-NMG.
Beaudoin, J. (2024). THE CDC MEMORANDUM: NOTICE OF CRIMINAL LIABILITY. Summa Logica LLC. Found at TheRealCdC.com.
Beaudoin, J. (2024). THE CONNECTICUT MEMORANDA SERIES Vol. I: NOTICE OF HOSPITAL HOMICIDE & ACUTE RENAL FAILURE DEATHS. Summa Logica LLC. Available only through direct inquiry to author.
Beaudoin, J. (2024). THE CONNECTICUT MEMORANDA SERIES Vol. II: COVID-19 “VACCINE”-CAUSED DEATHS & DEATHS FRAUDULENTLY LABELED “COVID-19.” Summa Logica LLC. Available only through direct inquiry to author.
Beaudoin, J. (2024). The Real CdC: COVID Facts for Regular People. Summa Logica LLC. Found at TheRealCdC.com.
Hi John, Regarding excess deaths per year, how do we distinguish the people who died from Sudden Acute Kidney Failure because they were given Remdesivir from those who died from Sudden Acute Kidney Failure from the COVID shot? For some, of course you might have a temporal proximity between the shot and the Kidney Failure. Since we know Remdesivir causes kidney failure why didn't you mention the Remdesivir issue in this post? The charts in this post cover 2021-2023 when both Remdesivir and the shot were "in play". Thank you for all your work!
The last 4 years have felt like I'm living in a bad dream and no matter how loud I scream or wave my arms, most can't sense my presence.