
Sudden Kidney Failure Began with COVID Treatment Protocols & “Vaccines”, not COVID
Forensic Investigation Required

[Third article in a series — Thank you, Dr. Meryl Nass, for the recommendation to break this into multiple articles. Here are the likely articles in the series. 1) Leadership, Management, and Strategic Planning in the Covid Era, 2) The Ineffective Messaging of “Myocarditis in Young, Male Athletes”, 3) Sudden Kidney Failure Began with Government Incentives, not with COVID, 4) Top-Down Investigation, Bottom-Up Quantification Method for Epidemiological Vigilance, 5) Differences in Pneumonia, COVID, and All-Cause Death Profiles by Age Group.]
Acronyms (alternates at end of article)
AKI - Acute Kidney Injury
CDC - Centers for Disease Control and Prevention
FDA - Food and Drug Administration
ICD - International Classification of Diseases
NCTAP - New COVID-19 Treatments Add-On Payment
NIH - National Institutes of Health
NIAID - National Institute of Allergy and Infectious Diseases
What caused and is causing a 100% increase in ICD code N17 Acute renal failure (aka sudden kidney failure, aka acute kidney injury) elucidated in the second article in this series?
The only way to conclusively answer that is to conduct forensic investigations of the medical files of decedents who died involving AKI. Data studies are only ever persuasive, not conclusive. For five (5) years in the COVID era, scientists, doctors, and armchair epidemiologists have been trying to find a smoking gun in the data. There isn’t one. Meanwhile, conclusive evidence lies in case reports like those collected by Aaron Hertzberg, or in the official government records compiled into THE CDC MEMORANDUM or THE CONNECTICUT MEMORANDA SERIES Volume II. Hundreds of pages of irrefutable testimony get little attention, while shiny objects like graphs capture the audience. Provocative headline statistics get millions of views on social media despite no ability to prove the conclusory statements accompanying the headlines. And all along, the conclusive evidence at the record-level remains ignored.
Pfizer documents are pored over by thousands of people for years in the hopes that the criminals will present evidence of their crimes on a silver platter. Government hoards and hides 1,000 times as many records as in the Pfizer trial data. Governments have more recent, more accurate, less corrupted, and more detailed evidence from “vaccines” than all the drug company trials combined. And all along, it remains ignored by the “experts” hunting data.
People, led by their social media harnesses, bantered about ineffective research papers and meta-analysis studies for half a decade in the COVID era. People on both sides are told to listen to “experts” rather than look down the street, talk to their extended families, or have conversations with workmates. The answers do not lie in the hero-worship of doctors. Most doctors have no training in what is needed for this COVID battle. The great war on The People is perpetrated by those who took power via a soft coup d’état and they use social media to control the narratives.
Some call me “the data guy.” Well, I hate data. I only do what no one else is doing out of necessity. Data is only a small fraction of the necessary “whole system” analysis required to de-puzzle the COVID era. Epidemiological modeling and methods are arcane, error-prone, and wildly inferential. Most of my analysis time is spent contemplating law, morality, philosophy, messaging and marketing, economic system efficiency, psychology, and sociology. COVID cannot be understood via biology, epidemiology, virology, immunology, statistics, or other “sciency" purviews. COVID was perpetrated on us using behavior modification flowing from propaganda, emotional blackmail, coercion, solicitation, and including threats to base level needs cued by purposefully constructed scarcities.
But, the game must be played, so here’s a response to the question in bold face type at the top.
Vaxophiles say that COVID causes AKI. Health freedom supporters are split between blaming COVID treatment protocols (including remdesivir and other drugs) and blaming COVID gene drugs rebranded as “vaccines.”
Persuasive evidence laid out in this article explicates three (3) strong conclusions. 1) COVID disease per se did not cause AKI involved excess deaths to a measurable degree, 2) COVID treatment protocols (Signal 1) did cause a significant percentage of AKI involved excess deaths, and 3) COVID gene drug therapies rebranded as “vaccines” (Signal 2) caused and are causing the other significant percentage of AKI involved excess deaths.
In this article, COVID is untangled from AKI in death records to show the timing differences in the signal. Did significant AKI excess deaths start when COVID started, when the hospital protocols started, when the hospital protocols were heavily incentivized by government payment plans, or when the COVID “vaccines” rolled out? These questions are explored in this article.
From the prior article in the series, excess AKI involved deaths 2021-2024 totals 211,802.1 This needed to be reiterated to understand the enormity of the iatrogenesis by some and murder by others.
When excess sudden kidney failure started
The timing correlates to two (2) separate and distinct signals. Signal 1 is seasonal (“on” in winter, “off” in summer). Signal 2 approximates a positive slope linear function that levels off at an excess steady-state.

Figure 1
The solid black line in Figure 1 depicts monthly totals of AKI involved deaths of all ages in Florida, a state of roughly 22 million people. The dashed black line represents AKI involved deaths after subtracting deaths also involving COVID. Thus, the dashed black line represents deaths involving AKI and not COVID.
The gray dashed lines in Figure 1 form a band of baseline normal from 2018 and 2019.
In early November 2020, the solid black line of deaths involving AKI inclusive of records with COVID rises above normal into excess never to return. In late December 2020, the dashed black line of deaths involving AKI, excluding records involving COVID, breaches normal into excess never to return to baseline.
Correlatively, 1) the New COVID-19 Treatments Add-On Payment (NCTAP)2 program aligns with the start of excess AKI inclusive of COVID and 2) the COVID “vaccine” rollout aligns with the start of excess AKI excluding records involving COVID.
The NCTAP program incentivizes hospitals to prescribe remdesivir and other NIH-recommended drugs upon a mere COVID positive test. The patient must be admitted to the hospital for five (5) days to run remdesivir via intravenous (IV) administration. The incentive as of November 2, 2020 pays an extra 20% of the entire hospital bill if remdesivir is used. In other words, if they can get a patient into the ICU for a million dollar invoice, then the hospital gets an extra $200,000 for running an IV of remdesivir based only on a positive COVID test and no other symptoms. The NCTAP is effectively a bounty put on the heads of COVID-positive patients.
Ideal example graphs
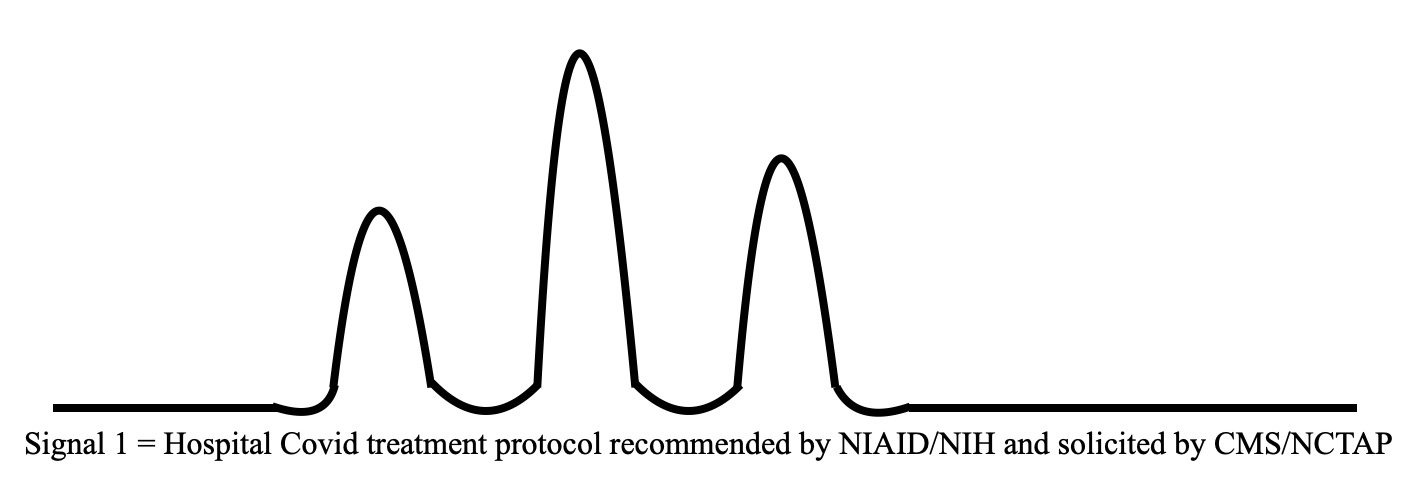


Figure 2
Figure 2 depicts what idealized graphs might look like.
Signal 1 (top plot in Figure 2) depicts a seasonal signal that returns to baseline in summers, which is what one would expect of a signal coincident with or resulting from COVID. People went to the hospital with COVID symptoms more in the winter and hardly at all in the summer. Thus, COVID hospital protocol involved deaths would mostly occur in the winter.
Signal 2 (middle plot in Figure 2) depicts what a vaccine rollout program might look like over time, except for the end. The initial steady-state zero signal ends upon introduction of a positive slope linear signal. Then the positive slope linear signal ends at a steady-state excess elevated far above the initial zero baseline signal. The actual “vaccine” uptake was likely not linear, but is probably close to it. Toward the end of the plot the signal did not fall from the excess steady-state as “vaccine” uptake fell off. If this is true in the actual signal, then this is probably the most pressing and concerning issue in all of COVID if these kidney failure deaths have not stopped. Yet governments are not investigating them. Excess All-Cause deaths also have not fallen as expected.
The sum of Signals 1 & 2 yield the third (3rd) plot in Figure 2. The black line plot of actual AKI involved deaths in Figure 1 appears quite similar to the combined signal in the bottom plot of Figure 2; and Signal 2 in the middle plot of Figure 2 appears similar to the dashed line actual AKI non-COVID involved deaths in Figure 1. Despite author bias in the creation of the idealized graphs, the theory of two (2) separate signals is compelling. The timing of events should be forensically investigated.
Most importantly, after subtracting COVID involvement, significant excess AKI involved deaths continued through 2021, 2022, 2023, and 2024. Signal 2 is apparent and stark. COVID is proven to not be significantly involved in the ongoing AKI involved excess deaths.
The sum of Signals 1 & 2 yield the third (3rd) plot in Figure 2. The black line plot of actual AKI involved deaths in Figure 1 appears quite similar to the combined signal in the bottom plot of Figure 2; and Signal 2 in the middle plot of Figure 2 appears similar to the dashed line actual AKI non-COVID involved deaths in Figure 1. Despite author bias in the creation of the idealized graphs, the theory of two (2) separate signals is compelling. The timing of events should be forensically investigated.
Most importantly, after subtracting COVID involvement, significant excess AKI involved deaths continued through 2021, 2022, 2023, and 2024. Signal 2 is apparent and stark. COVID is proven to not be significantly involved in the ongoing AKI involved excess deaths.

Figure 3
Figure 3 adds an adjustment for excess All-Cause deaths. 1) For each day of the nine (9) years, plot the 51-day rolling average (51RA) of AKI involved deaths as a percentage of the 51RA of All-Cause deaths as the solid black line plot. 2) For each day of the nine (9) years, plot the difference between the 51RA of AKI and the 51RA of COVID as the dotted line plot. For a detailed explanation of the Prevalence-of-Cause technique, refer to the article Prevalence-of-Cause (PoC) from July 18, 2024.
In the spring of 2020 in Massachusetts (Figure 3 middle plot) there is a small departure of the black line plot in excess of normal. Other than that, there is no signal of excess AKI in all three (3) states until November or December 2020.
Seasonality can be seen in all three (3) states especially in the 2021/2022 winter during which all three (3) show a clear gap between AKI involved deaths with COVID and without COVID. Clearly something was coincident with the seasonal COVID wave.
More significantly, the dotted line plot of AKI without COVID shoots up in early 2021 seeming to react to something well after COVID began its season. This is a second signal, Signal 2. Signal 2 can be easily seen by imagining a line drawn through the low points of the plots. Some externality causing AKI involved death is rising linearly to an absurdly epidemic holocaust level.
After looking at the northeast, southeast, and mid-west, below is a northwest state, Idaho, ranked 37th in the United States in population at just below two (2) million people.

Figure 4
Figure 4 depicts the same low grade excess AKI involved deaths beginning in late 2020. Then Idaho’s AKI excess explodes in August 2021, coincident with Florida in Figure 1 and not with the northeast and midwest states. This peak centered on October begins to ebb, but then peaks again characteristically as a normal seasonal wave centered in the winter of 2021/2022.
I picked Idaho because of the small population, remote location, and Top 5 conservative ranking among U.S. States.3 This is confirmation of a trend I have been tracking. There is no proof yet without individual surveys of hospital staff. The data favors that conservative states likely committed far less COVID record fraud and iatrogenic hospital protocol homicides than “progressive” states. The evidence is growing to support this, but I am not yet ready to defend this sociological study. Yet, there is evidence.
The colossal point of this article
The colossal point of this article is that COVID did not cause the excess AKI involved deaths and that there are two (2) distinct government caused reasons for the excess.
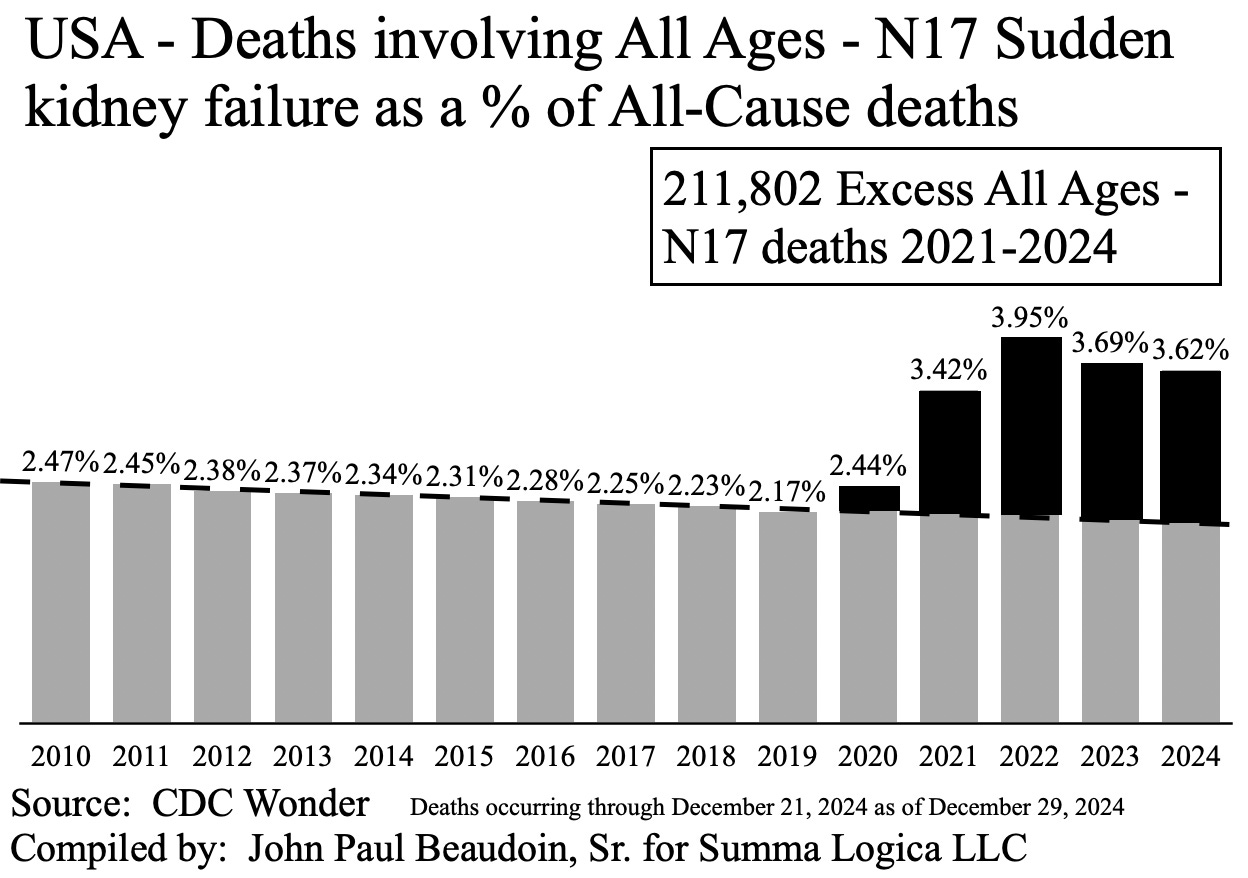
Figure 5
Figure 5 depicts AKI involved deaths as a percentage of All-Cause deaths for the whole of the United States. The government is trying to ignore this now, but this cannot be ignored by history. This article and many others from Coquin de Chien, The Real CdC, depict a real epidemic caused not by COVID, but rather by acts of man, by recommendations from NIAID including COVID drug and treatment protocols and COVID “vaccines.”
In order to lessen the possibility of confounding co-morbidities, a younger, healthier age group is now analyzed. Additionally, COVID involvement is also removed as a variable.

Figure 6
Figure 6 razes the counter-narrative purporting that COVID disease per se may have caused the AKI involved excess deaths. Id est, Figure 6 precludes COVID involvement. None of the records of decedents represented in this graph had U07.1 COVID-19 involved in their death records. Yet the excess is stark.
Years 2010 through 2019 in Figure 6 depict a highly deterministic trend over time. 2020 barely breaks that trend likely because of the November and December use of remdesivir. Excess deaths involving AKI ages 25 through 54 in the United States in years 2021 through 2024 total 15,095. How can people not exclaim this from the rooftops? What more evidence does anyone need that deaths from COVID disease are far less significant than deaths caused by government recommended COVID treatment and purportedly prophylactic gene drugs? In fact, government COVID recommendations killed more people who were far younger than those killed by COVID disease per se.
Conclusions
The excess deaths involving AKI seasonal Signal 1 began when remdesivir was heavily incentivized by CMS.gov. Remdesivir should be immediately suspended pending forensic investigation.
The excess deaths involving AKI steadily increasing Signal 2 began when COVID “vaccines” began. COVID “vaccines” should be immediately suspended pending forensic investigation.
AKI is involved in 211,805 excess deaths (2021-2024) in the United States at ages far younger than those from COVID disease per se.
Legal Duty to Act
The leaders of the NIH, FDA, and CDC have a legal duty to ensure that an earnest and immediate forensic investigation occurs using the medical files from decedents who died from AKI. There are no excuses. The omission of investigation is a felony failure of required legal duty to act. The People are dying and demand answers from our governments.
Strengths of conclusions
The ability to subtract COVID involvement, disambiguate a second signal from the data, and determine when Signals 1 & 2 each began are unique and persuasive conclusions.
If a disease causes a specific diagnosis of death, and there are excess deaths due to the disease, then the specific diagnosis should be involved in a higher percentage of All-Cause deaths than before the disease occurred. One of the strongest arguments lies in Figures 3 & 5 depicting AKI as a percentage of All-Cause deaths by year. Though COVID raged through 2020, AKI as a percentage of All-Cause deaths in 2020 is barely in excess. However, 2021 and after is clearly an AKI holocaust.
Weaknesses of conclusions
Data can be mistakenly entered, fraudulently altered, misunderstood, or be correct for the wrong reasons.
Recommendation
Data studies can only ever be persuasive evidence of causality. In order to conclusively prove to a clear and convincing or beyond reasonable doubt standard, the medical files of a representative set of decedents must be forensically investigated. The hourly vital signs, daily blood lab reports, imaging reports, digestive system inputs and outputs, medications and fluids administered orally and through IV recorded to the minute, and other information in the patient file must be used to build a timeline of events to determine which event caused or likely caused which issue.
Method Statement
The numbers used in this article are obtained from the U.S. government’s CDC Wonder database found at https://wonder.cdc.gov/.
Graphs labeled “United States” are built from data from the fifty (50) United States. Graphs labeled with a state name such as “Florida” are built from datasets from that specific state.
Determination of excess deaths:
excess deaths = actual deaths - expected deaths
expected deaths for a given period of time is calculated using baseline years 2010 through 2019 or from 2015 through 2019, depending on the graph. Approximate a trend line through the actual numbers from the baseline years. Extend the line through the target years (2020-2024). The points on the trend line are the expected values for each time period on the x-axis.
Examples using spreadsheet functions SLOPE and INTERCEPT, which use linear least squares algorithms.
Excess (March 2022) = actual value (March 2022) - (INTERCEPT({actual value (March 2015), actual value (March 2016), actual value (March 2017), actual value (March 2018), actual value (March 2019)}, {0,1,2,3,4}) + 7 * SLOPE({actual value (March 2015), actual value (March 2016), actual value (March 2017), actual value (March 2018), actual value (March 2019)}, {0,1,2,3,4}))
Notice the “7” as a coefficient to the SLOPE function. Year 2015 would be a coefficient of “0.” Year 2017 would be a coefficient of “2.” Year 2020 would be a coefficient of “5.”
If the baseline years were to be 2010-2019, then the second argument in SLOPE and INTERCEPT functions would be {0,1,2,3,4,5,6,7,8,9} and the first argument would use the actual values from those baseline years.
THE END (La Fin)
God Bless You All
John 14:6 TRUTH
References
Beaudoin, J. (2025 January 11). The Ineffective Messaging of “Myocarditis in Young, Male Athletes". The Real CdC. Found at https://therealcdc.substack.com/p/the-ineffective-messaging-of-myocarditis on 2025 January 14.
(Page Last Modified: 09/10/2024 06:27 PM). New COVID-19 Treatments Add-On Payment (NCTAP). Centers for Medicare & Medicaid Services. CMS.gov. Found at https://www.cms.gov/medicare/payment/COVID-19-vaccine-toolkit/new-COVID-19-treatments-add-payment-nctap on 2025 January 07.
(2024). Most Conservative States 2024. World Population Review. Found at https://worldpopulationreview.com/state-rankings/most-conservative-states on 2025 January 13.
Other References
Beaudoin, J. (2024). The Real CdC: COVID Facts for Regular People. Summa Logica LLC. Found at TheRealCdC.com.
Beaudoin, J. (2024). THE CDC MEMORANDUM: NOTICE OF CRIMINAL LIABILITY. Summa Logica LLC. Found at TheRealCdC.com.
Beaudoin, J. (2024). THE CONNECTICUT MEMORANDA SERIES Vol. I: NOTICE OF HOSPITAL HOMICIDE & ACUTE RENAL FAILURE DEATHS. Summa Logica LLC. Available only through direct inquiry to author.
Beaudoin, J. (2024). THE CONNECTICUT MEMORANDA SERIES Vol. II: COVID-19 “VACCINE”-CAUSED DEATHS & DEATHS FRAUDULENTLY LABELED “COVID-19.” Summa Logica LLC. Available only through direct inquiry to author.
Alternate Acronyms
AKI - A Cute Kidney Injury
CDC - Centers for Disease Creation and Proliferation
FDA - Federal Democide Administration
ICD - International Clusterfucation of Diseases
NCTAP - New COVID Treatment Assassination Payola
NIH - National Intent to Hex
NIAID - National Incentive to Allocate Inequity Disparately
Excellent and important. Thank you.
It’s increasingly obvious that Covid was created for the vax, not the other way ‘round.