
Chapter 14 Subsection (removed from book)
I49.9 CARDIAC ARRHYTHMIA INVOLVED DEATHS

In working with an editor, I agreed to remove most of the following text from my upcoming book, The Real CdC - COVID Facts for Regular People. The editor is correct in that it does not belong in the book. Rather than just discard it, I offer it here for the interest of doctors and others to discuss, correct, or comment upon. Thanks for reading. Life is short. Take chances. Make it interesting. Don’t just stay safe.
It’s also a teaser for the book because it’s taking me extra months in editing.
Many have seen cardiac waveforms on a heart monitor. The heart beats to a set of electrical signals that correlate to contraction and release of the heart muscle, which is the center of our circulatory system. If a signal for contraction occurs when the heart is supposed to relax, or vice versa, then the heart will fibrillate, which means that the smaller heart muscle fibers will twitch spasmodically, but the heart will not beat wholly and rhythmically.
The electrical system is confused by or confuses the autonomic muscular response of the heart. I write this as an engineer, not a doctor or biologist. My ideas are formed from conversation and from my engineering education.
Please view Figure 14.25. To avoid copyright issues, I drew it myself.

Figure 14.25
This is your heart depicted in voltage over time for each beat. You can see there are multiple waves and not just one rise per beat. The major parts of this signal, in order, are the P-wave, PR segment (flat line between), QRS-Complex, ST segment (flat line between), and T-wave. The PR interval includes both the P-wave and PR segment. The QRS Complex includes all sloped lines between P and T waves. Flat lines are not included in the QRS Complex.
All you really need to know is that if any of these signals changes in length of time relative to the others, then the heart may stop suddenly in fibrillation.
I learned a scant amount of this subject matter when I worked with someone who had Long-QT syndrome, a hereditary condition. Since March 2022, when I became aware of all the excess arrhythmia deaths, it seemed to me to be either an induced Long-QT-like issue or perhaps some other change to signal timing or delays.
In a conversation with Marc Girardot, Jessica Rose, Stephanie Seneff, and Kevin McKernan, Marc raised the issue of calcification of myocytes (cells of the heart’s myocardium) from apoptosis (the process of cell death). When cells die, they leave behind calcification. Kevin then raised the issue of the heart and electrical signals.
Lipid nanoparticles (LNP) or other substances in covid vaccines transfect or transform or transduce cells. Id est, they work themselves into the cells. The human cells sometimes react to the foreign substance with an allergic inflammatory response due to the cell not recognizing the infiltrator as a human substance. The trigger to the inflammatory response could be any of the phospholipids, polyethylene glycol (PEG), or it could be the a glycoprotein (spike protein) produced by translation of the mRNA payload released from the covid vaccine’s LNP’s that got into the human cells.
Scientists and doctors do not definitively know all that is happening. Personally, I believe there are multiple mechanisms of action occurring, thus confounding the research. But there is one sure thing. It is happening in a great number of people.
People seem to be randomly selected by fate in a Death Lottery. It could be an IV (intravenous) mistake (accidental injection into a blood vessel) or simply the person’s body chemistry is averse to something in the covid vaccine, or perhaps the genetic make-up of the recipient precludes symbiosis with this new technology. You may react and you may not. No one knows the odds, but it seems to me by the data to be more than one in one thousand die from a covid vaccination. Most are over 85-years-old. Thus, few relate the causation of death to vaccination without the advantage of massive amounts of data analyses, such as are presented in this book.
Perhaps I find this electrical signal topic important because my education is in electrical engineering. Arrhythmia and more specific diagnoses such as Long-QT and PR interval issues have much to do with the electrical system. Resistance, capacitance, and inductance combine to form an impedance circuit network. Whenever the impedance changes in part of an electrical circuit, the waveform changes. The delays or amplitude or frequency of the circuit can change.
Imagine if some myocytes (heart myocardium cells) become transfected, inflamed, experience apoptosis, die, and leave calcium behind. Calcium is actually a very good conductor. I was surprised when I looked it up. If there is a short circuit in any of the pathways of electrical conductivity from the sinus node to the ventricles, then the rhythm of the heart may be altered.
Another hypothesis is that the autonomic system is dysregulated by deleterious covid vaccination effects and that is the cause of irregular heartbeats.
Further imagine an issue unnoticed during normal life. The issue is a PQRST change due to inflammation, calcification, or dysregulation. The issue could result in fibrillation when sleeping deeply about an hour before waking up; or when the heart is most stressed from an adrenaline burst after a drive to the hoop, a run down the first baseline, a tangle in the box just before letting one rip into the lower right corner, or any play in an American football game. Another theory about the “died in his sleep” deaths is that the body will produce a large amount of adrenaline to wake a person up in the morning. It seems to be preparation to get everything moving again.
Though I am not a doctor or biologist, I believe the impedance characteristics of the heart are being altered and are unnoticed on regular exam or it is a neurological autonomic system issue possibly from myelination changes due to a covid vaccine. Figure 14.26 shows annual deaths involving arrhythmia.

Figure 14.26
The All-Cause, Covid, and Pneumonia (ACP) pattern of excess is broken again in Cardiac arrhythmia involved deaths as it is in Cardiac arrest and Pulmonary embolism involved deaths.
Years 2021 and 2022 cardiac arrhythmia involved deaths are greater than in 2020. ACP all went down, while Cardiac arrhythmia involved deaths went up from 2020 to 2021.
Cardiac arrhythmia involved deaths is another inverse relationship to ACP.
The excess deaths in 2021 and 2022 total 488 people who had families and friends who cared about them.
Will year 2020 Cardiac arrhythmia involved deaths fade into the baseline trend of 2015-2019 after normalizing for total All-cause deaths in each year? Figure 14.27 shows the percentage of total All-cause deaths each year involving Cardiac arrhythmia.
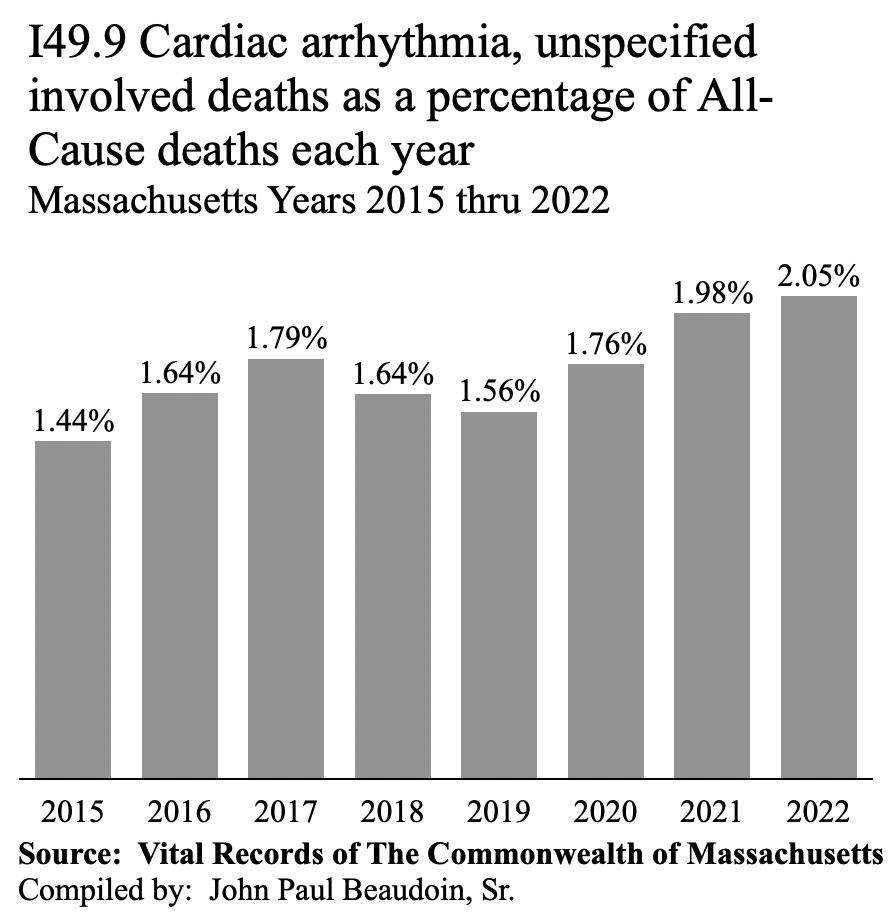
Figure 14.27
In Figure 14.27, the major increase in 2020 Cardiac arrhythmia involved deaths all but disappears when adjusted for All-cause deaths. In fact, 2017 is greater than 2020, and 2016 and 2018 are close to 2020.
There is no question that something bad happened in 2021 and 2022 causing Cardiac arrhythmia involved deaths.
EXHIBIT F of Beaudoin v Baker et al (2022) contains several pages of “CARDIAC DYSRHYTHMIA” causes listed in Part I of many Death Certificates of young people.1
I conducted a data study and investigation for someone who wished to challenge university vaccine mandates. I filtered 2021 and 2022 deaths for ages 18 to 22. I remember more around half having “CARDIAC DYSRHYTHMIA” as a cause of death in those two years. I was too sad to continue and I didn’t want to get into 2015 - 2019 of that age range because my son is in that age group in the 2018 database. I cannot look at his record.
The timeline in Figure 14.28 will tell us when the Cardiac arrhythmia involved deaths occurred.

Figure 14.28
In Figure 14.28, there appears to be a diminutive seasonality signal for cardiac arrhythmia involved deaths in most baseline years. The only two noticeable bumps are winter 2021/2022 and spring 2020.
Interestingly, Cardiac arrhythmia involved deaths in the year 2020 is also above normal all year long, not just in spring 2020. But the year 2020 did not start that way. It was among the baseline years until March 2020, when everyone became scared of covid and government mandates were put in place in May 2020. Unlike ACP, cardiac arrhythmia did not ebb into normal after the first spring wave. It stayed at a higher rate than baseline years 2015 - 2019 all year long.
Nearly five hundred excess arrhythmia deaths in the two years 2021 and 2022 from one cause of death is significant. One tenth of that was enough to stop vaccine rollouts nationwide in the past. This is one state, one single cause of death, and is ten times more than nationwide numbers that stopped prior vaccines. This is more evidence that nothing was going to stop this vaccine from rolling out. The Department of Defense deployed Operation Warp Speed on The People regardless of the harm known to occur by February 2021. Diane Dubois died in March. Brianna McCarthy died in April. Eden MacDonald died in June 2021. And they still continued to push covid vaccines and restrict the free of any questioning voice.
MA DPH probably still does not even track or know about the stark increase in Cardiac arrhythmia involved deaths.
Figure 14.29 depicts Cardiac arrhythmia age groups.

Figure 14.29
Please view each age group in Figure 14.29 in context of the other graphs. Clearly something killed more people by Cardiac arrhythmia in 2020 when there were no covid vaccines. Even though adjusting for All-cause deaths in Figure 14.27 showed that year 2020 all but disappeared into normalcy, that does not explain the 25 to 44 aged group being relatively so much higher than 20215 - 20019 baseline years.
If covid was cut in half from 2020 to 2021, why are most Cardiac arrhythmia death age groups much higher from 2020 to 2021? And why is 2022 highest? ACP all went ‘down’ from 2020 to 2021, while Cardiac arrhythmia went ‘up.’ The trend is the inverse.
Correlation across variables is warranted.
In 2020-2022, there were {10219, 5579, 4318} U07.1 covid involved deaths, {1216, 1267, 1318} I49.9 Cardiac arrhythmia involved deaths, and {36, 49, 53} deaths involving both.
The percentages of covid involved deaths that also involved Arrhythmia in 2020-2022 are {0.4%, 0.9%, 1.2%}. This tripled in only two years. What is the probability that covid deaths with arrhythmia would be 3X in two years? Something is very wrong with the recording of deaths by cause in Massachusetts.
The percentages of Arrhythmia involved deaths that also involved covid in 2020 - 2022 are {3.0%, 3.9%,4.0%}.
Given all the fraud uncovered and factually documented in PARS UNA and PARS DUO, it seems that covid-vaccine deaths involving Cardiac arrhythmia may have been labeled as covid deaths, when covid had little to do with the death.
With access to a certain state database, I would be able to determine to a great degree if covid vaccine deaths by Cardiac arrhythmia were labeled as covid deaths, while omitting any mention of covid vaccines. This discussion expands in a later chapter.
AUTHOR’S NOTE
One theory is that having covid before vaccination acts as a dose. The body is primed. Thus, the first dose of an actual covid vaccine is essentially the second encounter. The body may react adversely to dose 1 of the vaccine having been primed by covid. This is a very plausible theory that the data seems to support. Thus, covid is causal in the death, but only because a covid vaccine was given. The vaccine and covid could then be actual and proximate causes, or more likely would be called “substantial factors” in law. However, the covid vaccine might possibly be considered a superseding cause in legal terms. Legal terminology aside, practically, covid could be included on the Death Certificate if the death certifier knew that covid and the covid vaccine were required together to kill the decedent. This guesswork would not be necessary if the Massachusetts Department of Public Health or the CDC simply did their jobs and examined the data available to them that they hoard and obfuscate.
BONUS GRAPHS - THESE TELL QUITE A BIT BY AGE


I cannot express how brilliant you are. THe lottery essays, all the work on digging into the Mass statitics, and then this.
My hat is off to you. You sir, have a genius mind.
Honored to "know" you on Substack.
I to cannot get enough of this brilliant work!